

Endometrial carcinoma, or endometrial cancer, is when malignant or cancer cells arise in the glands of the endometrium, the lining of the uterus. The uterus is a hollow organ that sits behind the urinary bladder and in front of the rectum. The top of the uterus above the openings of the fallopian tubes is called the fundus, and the region below the openings is called the uterine body. The uterus tapers down into the uterine isthmus and finally the cervix, which protrudes into the vagina.
There any many grooves in the stroma
which is lined by the epithelium and these are the uterine glands that secrete
a glycogen-rich fluid that’s essential for the developing embryo during early
pregnancy. Endometrial carcinoma involves the abnormal growth of the epithelial
cells that make up endometrial glands, and there are two main types. The most
common is Type 1 endometrial carcinoma, which is also called endometrioid
carcinoma because the tumors grow in a way that looks like normal endometrial
glands. It usually involves several genetic mutations in endometrial cells,
including PTEN, a tumor suppressor gene; PIK3CA, an oncogene; and ARID1A, a
gene regulating chromatin structure. All of these mutations increase signaling
in the PI3K/AKT pathway, which promotes the growth and replication of endometrial
cells. More signaling in the PI3K/AKT pathway also enhances the expression of
genes that are linked to estrogen receptors.

Age is also a factor since endometrial carcinoma tends to develop in women who have gone through menopause, usually around 55 to 65 years of age. Finally, a hereditary condition called hereditary nonpolyposis colorectal cancer, also called Lynch syndrome, causes a high risk of developing certain cancers, including colon cancer and endometrial carcinoma. The good news is that there are actually factors that protect against Type 1 endometrial carcinoma! Taking hormonal contraceptives, being older at the time you give birth, and breastfeeding all reduce the risk of developing this type of cancer. Now, type 2 endometrial carcinoma is rarer and has a number of subtypes. The most common subtype is serous carcinoma. The genetic mutations found most often in serous carcinoma involve the TP53 gene, another tumor suppressor, aneuploidy, or an abnormal number of chromosomes after cell division. Type 2 carcinomas don’t appear to be linked with estrogen levels. These cancers typically affect women who have endometrial atrophy and who have lower body weight. They also tend to develop later in life than Type 1 and are more common in women of African descent. Even though there are two distinct types of endometrial carcinomas, we use the same stages to describe their development.
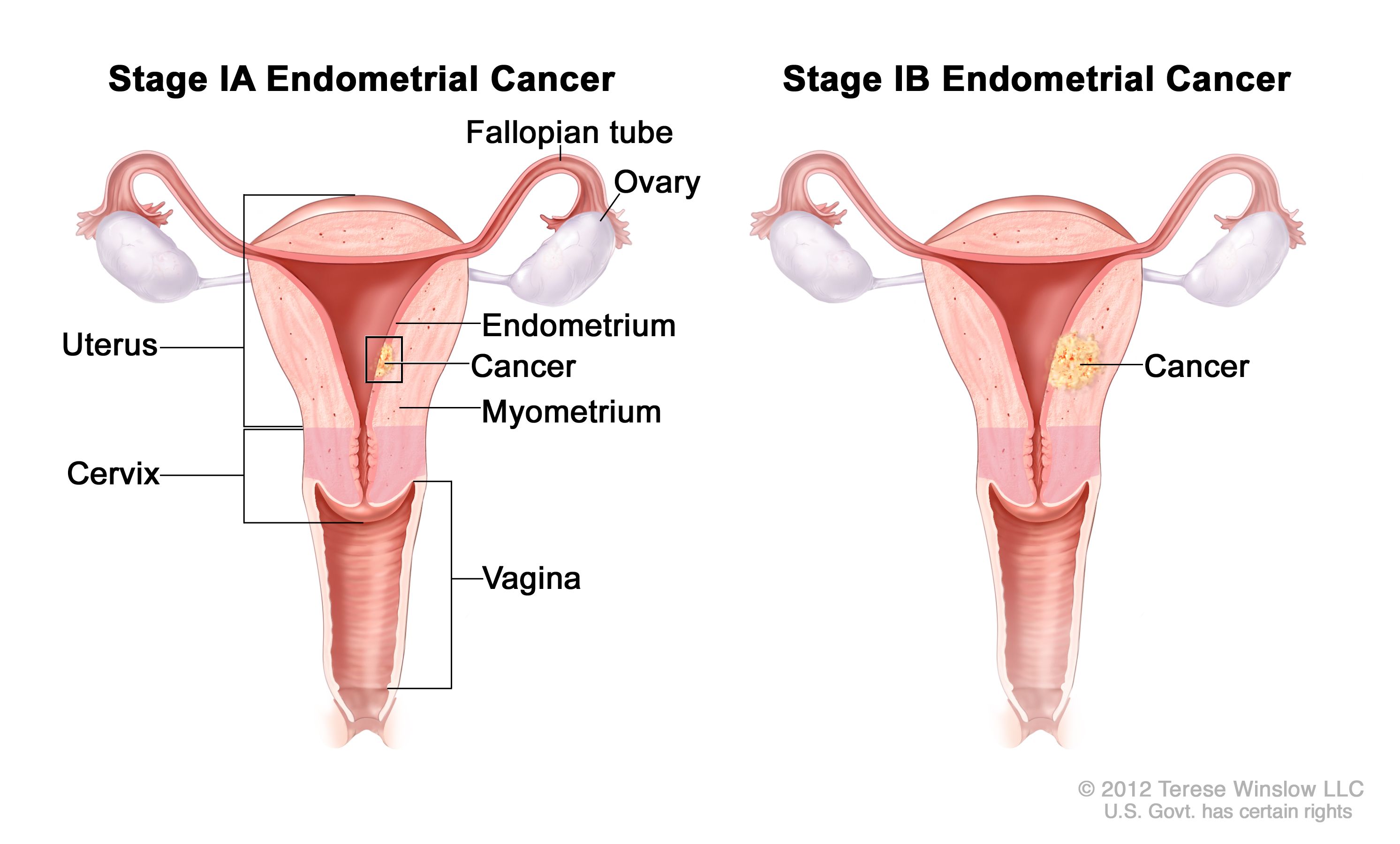
In stage 1, the carcinoma is only in
the uterus.
In stage 2, it has spread to the
cervix.
In stage 3, it has spread outside
the uterus but is still within the lesser, or “true” pelvis.
This means it could affect
structures like the vagina and pelvic lymph nodes.
In stage 4, it has spread beyond the
pelvis.
Most Type 1 endometrial carcinomas
are diagnosed in stage 1 and aren’t very aggressive, and because of that, they
have a good prognosis. But type 2 carcinomas are trickier and much more
aggressive and often spread to other body parts via the lymphatic system
or the fallopian tubes. The main symptom of endometrial carcinoma is abnormal
vaginal bleeding, usually without pain.

All right, as a quick recap,
endometrial carcinoma is a very common cancer of the lining of the uterus. Type
1 is associated with having abnormally high levels of estrogen over a long
period of time and is usually preceded by endometrial hyperplasia. Type 2,
which has several subtypes, isn’t linked with estrogen levels and is more
aggressive than type 1. The most common symptom is abnormal vaginal bleeding
after menopause and the treatment is hysterectomy with bilateral
salpingo-oophorectomy.